
My birth story as a Mum with type 1 diabetes
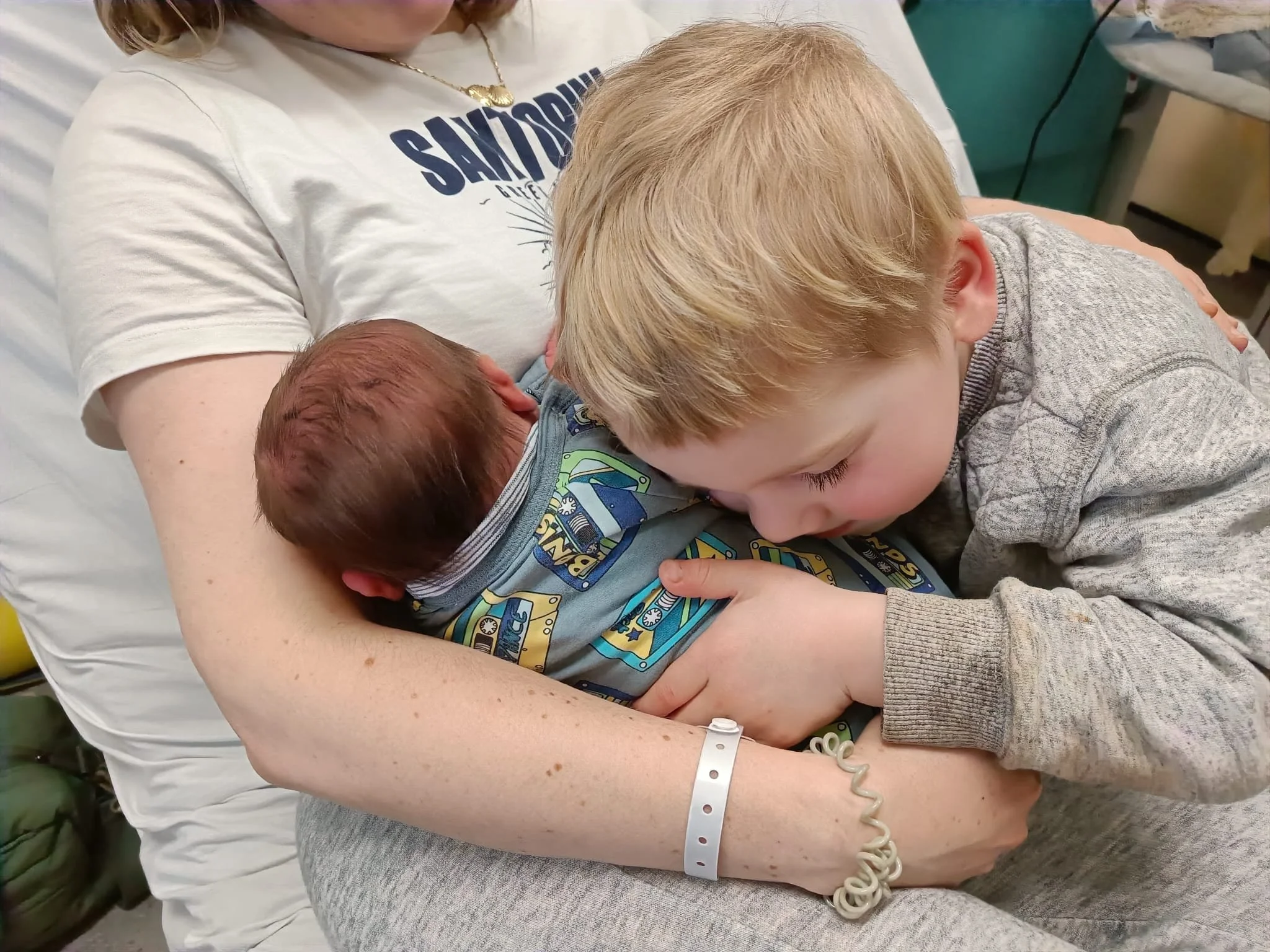
In early February, I gave birth to my beautiful baby boy, Max. He was healthy, and I ended up with the birth I really wanted - not a guarantee given the capricious and unpredictable nature of bringing new life into the world.
In early February, I gave birth to my beautiful baby boy, Max. He was healthy, weighing 8lbs 2oz (3.7kg) and I ended up with the birth I really wanted - not a guarantee given the capricious and unpredictable nature of bringing new life into the world.
And after many anxiety-inducing months of navigating a ‘high risk’ type 1 diabetes pregnancy, I was beyond relieved to have him here, and for him to be well. Whilst overall my experience was a positive one, there were plenty of twists and turns to keep us on our toes, and a fairly difficult postnatal experience in hospital - more on that below.
For now, he’s here, and 8 weeks down the line, I want to document what happened, as a personal journey for myself (that we did it!) but also to serve as a hopeful reassurance that women with type 1 diabetes can have healthy babies, and can get the birth they wish for.
Buckle up, it’s a chunky one.
Antenatal concerns
To begin, we need to start in January, a few days after the new year, and me well into my third trimester. I’d been back and forth to the triage and antenatal clinic. My insulin requirements had dropped a fair amount in the last 4 weeks of pregnancy. This isn't expected. Usually you’re busy chasing down highs due to increasing resistance. As the placenta is responsible for providing the hormones that cause insulin resistance, there were concerns that my placenta was ageing too much or too quickly, and wasn’t working well enough to provide the baby with all the nutrients and oxygen he needed. This is more likely to happen if you have type 1 diabetes.

Overnight stay at triage featuring very sexy compression stockings (& lots of Bridgerton)
That being said, the frequent growth scans showed good blood flow between my placenta and the baby, and the baby was growing in line with what was expected. It was hard to understand the shift in insulin requirements, and plethora of hypos.
During one of my final antenatal appointments at 36 weeks, due to concerns around hypos and lower insulin requirements, in the room with me I had two obstetricians, 1 DSN, 1 diabetes consultant, 1 midwife, and a diabetes dietician, all trying to fathom what could be going on. Despite the stress, this was a really useful appointment as it truly felt like collaborative care between me and the medical professionals. My insights were just as useful for developing a plan that felt good for all of us. Though none of us could really work out what was happening.
Due to the stress and concerns around the pregnancy (at one point, there was talk of delivering there and then), my blood pressure spiked high. Not uncommon to happen during stressful times, but due to my history of developing pre-eclampsia during my last induction, and the increased likelihood of high BP in T1D women, I landed myself an overnight stay in the triage ward. I started on the first line treatment for hypertension in pregnancy (a medication called labetalol) and settled in for 4-hourly observations. Babe was monitored on the CTG and he looked happy and content.
My BP seemed to stabilise with the medication, and a calmer nervous system. In the morning I was sent home, but recommended to start the induction sooner than planned. Not completely unexpected, and frankly welcomed by me after all the ongoing uncertainty.
Induction
On Sunday 8th at 4pm, I was admitted to the induction ward. The midwife looking after me had a special interest in type 1 diabetes, which automatically put me at ease and honestly makes all the difference to hospital care. We talked through different induction options. I’d used the hormonal pessary with my first induction, and was keen to go for this again. Even though it hyper-stimulated my cervix and caused some issues with back-to-back contractions, I was willing to overlook that because it got the job done.
However, it turns out my keen bean cervix wasn’t a fluke. The hormonal pessary is known to hyper-stimulate and cause problems. Given my history, my midwife dissuaded me from the pessary and recommended the cook balloon instead. This involves attaching two balloons filled with saline to your cervix and vaginal. It’s non-hormonal and uses gravity to irritate the cervix into action - so more reminiscent of a spontaneous labour.



At 6pm, and with a healthy dose of gas and air, the cook balloons were inserted (the least fun kind of balloon, as my friend texted me, in sympathy). Now I had to wait for 24 hours, or for the balloons to fall out, whichever came first. I was told to keep mobile and positive, cue lots of bouncing on a pregnancy ball and lots of baths. I also roped my husband into daily back massages to keep my hypertension at bay. So far so good.
Overnight, I started to feel some tightenings and discomfort and was getting excited, but by 6pm the next day, the balloons were still in place and they had to be manually removed. I was only 2cm dilated. The next step on the intervention pathway was to break my waters, but I needed a room on the delivery suite for that to happen. So we hunkered down for another 24 hours on the induction ward (more massages, baths…so wasn’t all bad).
By 10.30pm the following day, after a listless day of waiting and much money spent in the hospital’s M&S, we finally got the green light to head up to the room where I’d give birth. Once there, we discovered there were some concerns with the baby’s positioning. He was still high (didn’t my ribs know about it), so they recommended performing a controlled rupture of the membranes. This meant having two midwives present. One to break my waters and the other to push down on my stomach, encouraging the baby's head to descend before the umbilical cord could (it’s rare for the cord to get there first, but if this happens it’s a medical emergency).
Given the busyness of the ward, we had to wait until 3am for this to happen. Not a problem as it allowed us to rest a bit, though of course, I was too nervous to settle.
As soon as the waters were broken (basically with a big hook that looks like a knitting needle - nice) my contractions really ramped up. They were coming every 90 seconds to 2 minutes. It was undeniable that things were progressing now.
Active labour
I used breathing techniques and pacing around the room to manage for the first hour or so, but I felt quite out of control with how quickly things were happening. My midwife was fairly hands off, and she spent a lot of time sat in the corner taking notes. I guess I wanted more encouragement and reassurance from her, but in the moment couldn’t find a way of communicating this.
I started using gas and air, and my plan pre-induction was to use this throughout, as I had done with my first labour. But this time, and probably because I necked it all a bit too quickly, the gas made me nauseous and I started to vomit. I panicked and started to doubt I could do labour if my pain relief option wasn’t viable.
Despite the intensity of the birth, diabetes-wise things were looking incredibly smooth. I was managing using the CamAPS system (hybrid closed loop pump - more on those here). I was fully prepped with hypo treatments (Lift shots), and was ready to hit the Boost function as soon as necessary. I’d given my husband a crash course in t1d management, so as well as being my birth partner, he was also my assistant pancreas. Hats off Eddie!
But as it turns out, I didn’t need to do any of those things. Yes, the irony of diabetes pushing me into the ‘high risk’ category but causing me no problems is not lost on me.
I managed a few intense rounds of contractions before requesting a vaginal exam. I was 5cm. This was a blow. I felt much further along - maybe wishful thinking? - but I guess it brings up a valid discussion of how useful exams can be. 5cm knocked my confidence. I felt way more than 5cm. So I decided to opt for an epidural. Luckily for me the anaesthetist came quickly, but it took longer than expected to insert. The contractions were coming so quickly, so we had to wait until they passed for the doctor to insert the catheter into my back. Finally it was in and I could move positions.
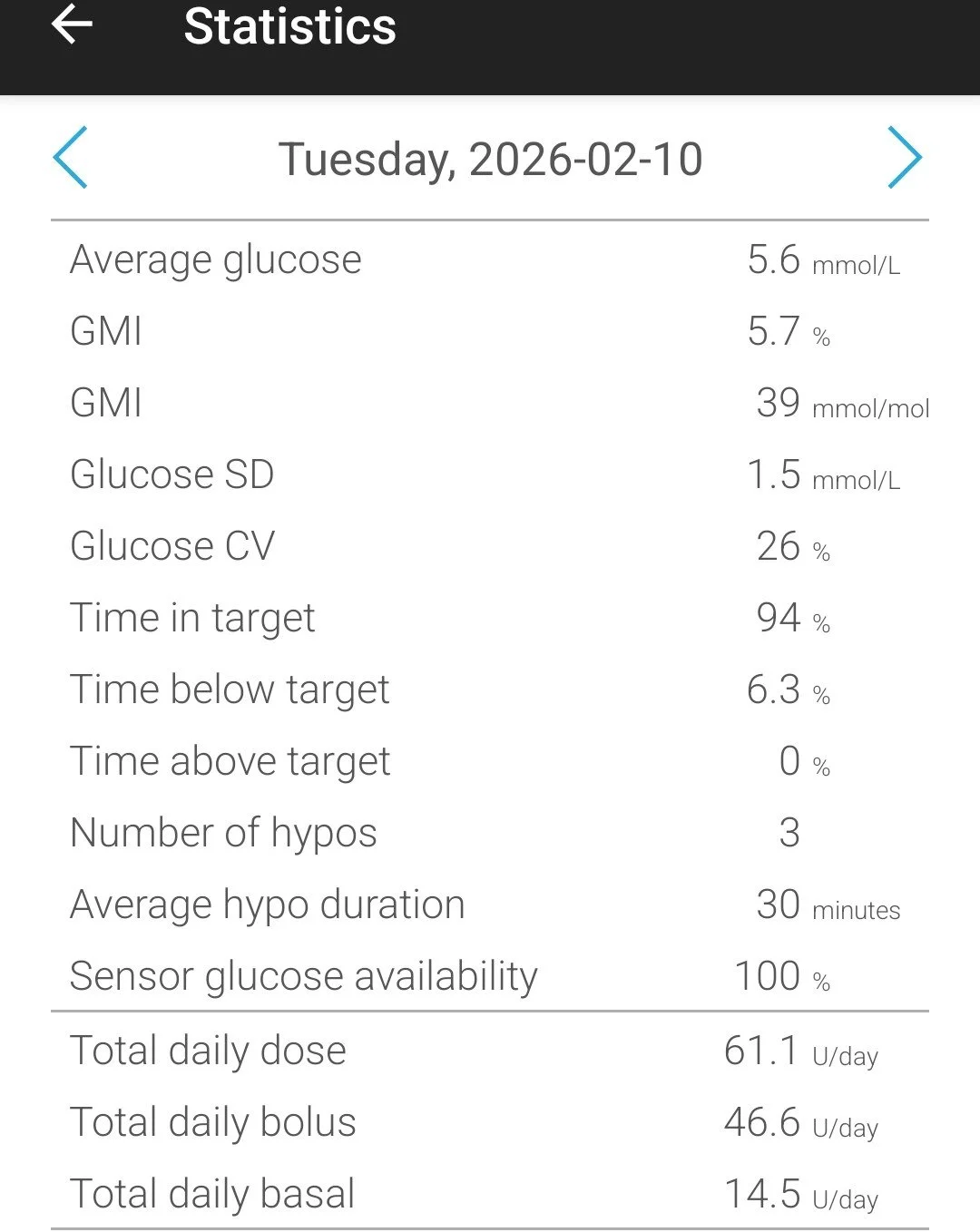
Stats from my pump the day Max was born
now push it🧡
push it real good 🧡
now push it🧡 push it real good 🧡
Time to push
Time gets very hazy here, for both me and my husband, but it felt like the process from epidural insertion to feeling the urge to push was a blink of the eye. A more senior midwife entered the room at this point, I think at the bequest of my midwife, not me, but I was happy she was there. She was assertive, and direct, and she could see that I was ready to push. She asked to examine me, announced I was 9.5cm, and that as I’d had a baby before, ‘could push the rest of the cervix away’. This kind of matron-esque, no-nonsense vibe was just what I needed.
She helped me get into the best position and talked to me calmly and clearly.
My baby was still high up, and he didn’t like the position he was in. A subtle yet powerful message - you need to act.
I remember the intensity of pushing and gritting mg teeth - no idea how long this went on for. I struggled to feel him move down, maybe due to the epidural, but he made his way. Two more midwives came in. It was the morning handover. I was happy for them to be there, I wanted that cheerleading.
I remember someone suggesting I boost the epidural and then that was it, I gave another push and his head was out. There was quite a reprieve before his body followed, and I found that time odd. The midwiveskept saying how close I was, and encouraging me to go again. I felt like I was miles from the finish line, even though I could feel his head. I turned to my husband for the truth. And he smiled, held my hand, and said, you’re almost there.
That was all I needed before I went one more time, and at 7.38am, about 4.5 hours of active labour, Max was scooped up and placed onto my chest.
We had a beautiful golden hour together. Unhurried, calm, peaceful. The cord was only cut once it had stopped pulsating. We had our first breastfeed. I birthed the placenta.
Side note on the placenta - it was huge. Something I found out later, is that T1D women grow large placentas which have fewer blood vessels than any other pregnant group. This is called hyperplacentosis. It’s also why 150mg of aspirin is prescribed - to reduce the amount of platelets in circulating blood so that those fewer vessels get as much blood as possible. It’s also why our babies be plethoric - have more red blood cells - and are prone to jaundice.
Postpartum care
Max’s blood glucose levels post-birth were always fine. There can be a risk of babies’ glucose being low due to the insulin they’re exposed to from Mum. But as is standard care, his levels were checked for 24 hours post birth. I felt good, minimal blood loss and a few stitches that I didn’t feel due to the epidural. We got moved to a private bed on a transitional care ward. This is a special ward, a step down from NICU, for babies and mothers who are seen as high risk.
I loved this ward. True continuity of care, lots of support, privacy and space.
After 24 hours, Max got discharged, but due to an abnormal kidney function test result, I wasn’t cleared to leave. So we stayed in for another 24 hours. The next day, my bloodwork was fine, but Max developed jaundice (see above point re. placenta). I was heartbroken. Even though it’s very common, I felt as though he wasn’t getting enough food from me to flush out the bilirubin. There are different levels of jaundice and Max reached the threshold for phototherapy treatment. This required him to be in a hospital incubator for 24 hours, so blue-green light could be shone on him to break up the excess bilirubin. He was only allowed out every 3 hours for feeding, and feeds should last no longer than 15 minutes, to maximise the light exposure.
At the same time, someone with greater need than us needed our room, so we got moved to the standard post-natal ward. We found ourselves on a busy and noisy 6-bed bay, sleep deprived, with an inconsolable baby that we couldn’t console. At this point, my husband became invisible too. I found the phototherapy treatment hard to go through, and it gave me a very very tiny insight into how agonising it must be to have a baby on the NICU. The medical team around me didn’t really understand my distress. As far as there were concerned, they’d diagnosed the problem, and had set up the correct treatment to fix it. I didn’t need to be upset.
Being on this ward took me straight back to the postpartum experience I had with my first child, which was arguably one of the toughest times of my life. I had pre-eclampsia and my son was poorly. So on paper a lot more challenging than this labour and postpartum, but my body didn’t seem to distinguish between the experiences. I guess because the lights, the noise, the busyness of the ward, the worry, all took my nervous system right back. The hypertension that up until that point was being managed successfully on medication, soon went out of control and no longer responded the the meds.
I ended up being on the postnatal wards for 8 days, as we all tried to manage the high blood pressure. Luckily, by the final few days, I’d got my own private room, and most midwives knew me pretty well, so at least I developed my own continuity of care by sheer dint of being there so long. The medics increased my dose, changed my medication, added in more medication, but still, as soon as I heard that blood pressure machine wheeling its way down the corridor to me, my body panicked and my BP increased. I was under 4-hourly observations, and I needed to have at least 24 hours of reasonable blood pressure readings before I could go home. This task seemed Sisyphean.
But, after the support of a really great midwife and doctor, on a soggy, grey February afternoon, a whole 10 days after being admitted to hospital, we were given the green light to go home.


Reflections
I feel immensely grateful that I had the birth I wanted. I feel so lucky that my son was, and is, healthy. I feel grief that the beginnings weren’t what I wanted. I’d hoped the postpartum experience would heal the trauma from my first child’s birth, and it didn’t. I had to sacrifice part of our breastfeeding journey so I could concentrate on managing my blood pressure. I ached for my first-born child too, as we’d never been apart that long before. As someone who doesn’t live her life feeling ‘high risk’ being seen through this lens is always tough. Undergoing regular blood pressure checks that told me how poorly I was every 4 hours, was sobering and jarring. I don’t see myself as sick, fortunately.
But despite the twists and turns, I am well and I feel well. Above all, I’m proud, and I hope I’ve shown you that you can have a positive pregnancy and labour experience with type 1 diabetes. Maybe even your positive experience is not despite type 1, but because of it.
If you have any questions or comments, I’d love to hear them! Let me know below.

The T1D Pregnancy Companion
A thorough guide that meets you wherever you're at on your type 1 diabetes fertility journey
The T1D Pregnancy Companion
ALSO - if you’re reading this and hope to have your own t1d pregnancy, but feel overwhelmed, I’ve developed a resource for this exact this moment in your health journey.
To replace fear with facts, and confusion with confidence.
It's a thorough guide that meets you wherever you're at on your type 1 diabetes fertility journey.
Full of evidence-based recommendations, practical interventions, and a toolkit that looks after your mind just as well as it looks after your time in range.